Virtual Endoscopic Surgical Simulator Aims to Improve Surgical Training
Colorectal cancer is the third most common cancer for both men and women in the United States and the second leading cause of cancer-related deaths. Endoscopic Submucosal Dissection (ESD) is often used to resect premalignant or early-stage lesions. This procedure involves injecting fluid beneath the lesion, causing enough separation from the submucosal layer to allow easier dissection. Unfortunately, performing ESD can be very challenging, and most hands-on training occurs in the operating room. To help alleviate these problems, CeMSIM (RPI) in collaboration with Beth Israel Deaconess Medical Center in Boston and Kitware, is developing a virtual endoscopic surgical simulator (VESS). VESS is a virtual reality-based trainer with haptic feedback, allowing surgical trainees to attain competence performing ESD in a controlled environment with no risk to patients. The simulator provides customized learning, real-time feedback, mentoring, and objective assessment to improve future surgical outcomes.
Building VESS Using Kitware’s Interactive Medical Simulation Toolkit (iMSTK)
VESS was built on iMSTK, Kitware’s open source toolkit that aids with rapid prototyping of interactive virtual surgical simulations. iMSTK provides a rich feature set for surgical simulators, such as real-time physics, haptics, collision detection and response, (external) hardware support, and advanced rendering.
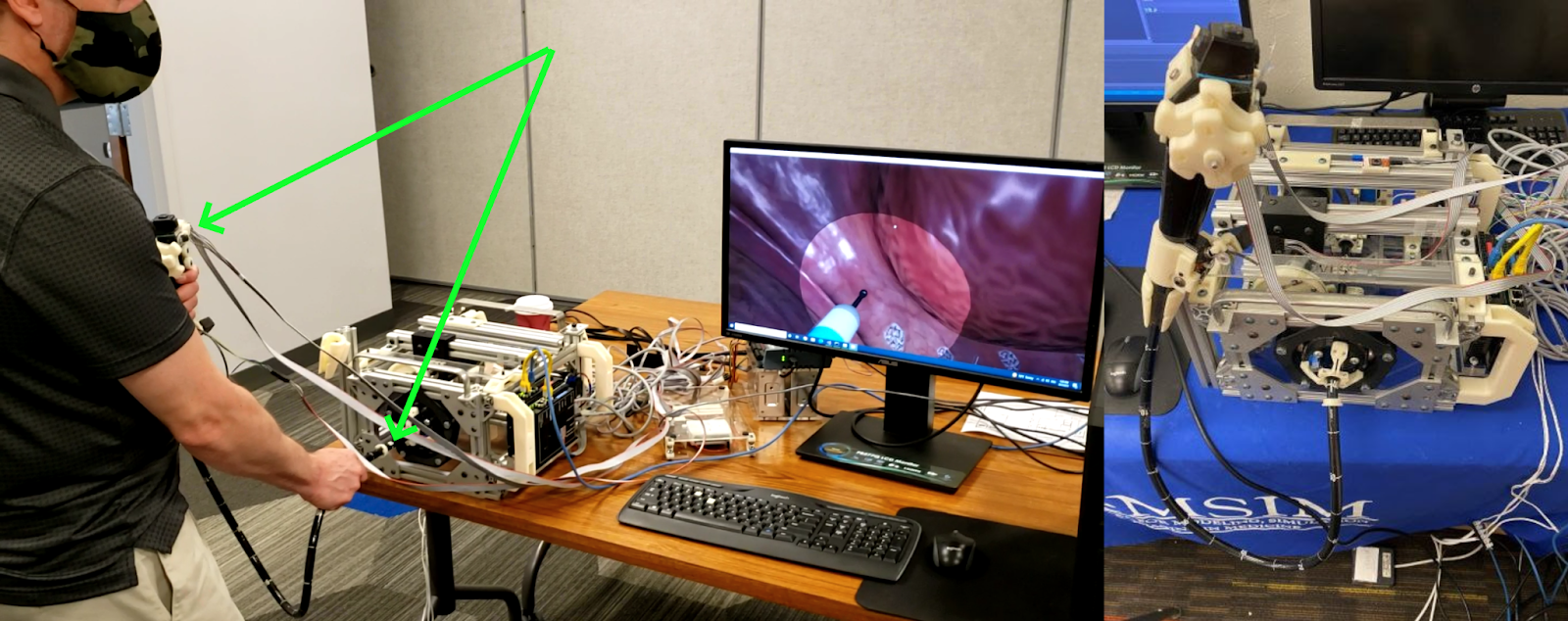
CeMSIM developed the custom hardware that mimics the endoscopy setup in the operating room. This interface features a scope that can be slid along the scope axis as well as twisted for rotational control. The U/D and R/L angulation knobs on the endoscope body control the other two axes of rotation through mechanical angulation of the head of the endoscope (see Figure 1). The scope is designed to provide realistic frictional resistance to the motion of the real scope. iMSTK’s highly extensible hardware interface classes allowed us to easily interface with this hardware, despite it being a fully customized build. The software is responsible for tracking and displaying scope movements, real-time tissue dynamics, collision and contact simulation, and photo-realistic rendering.
VESS In Action
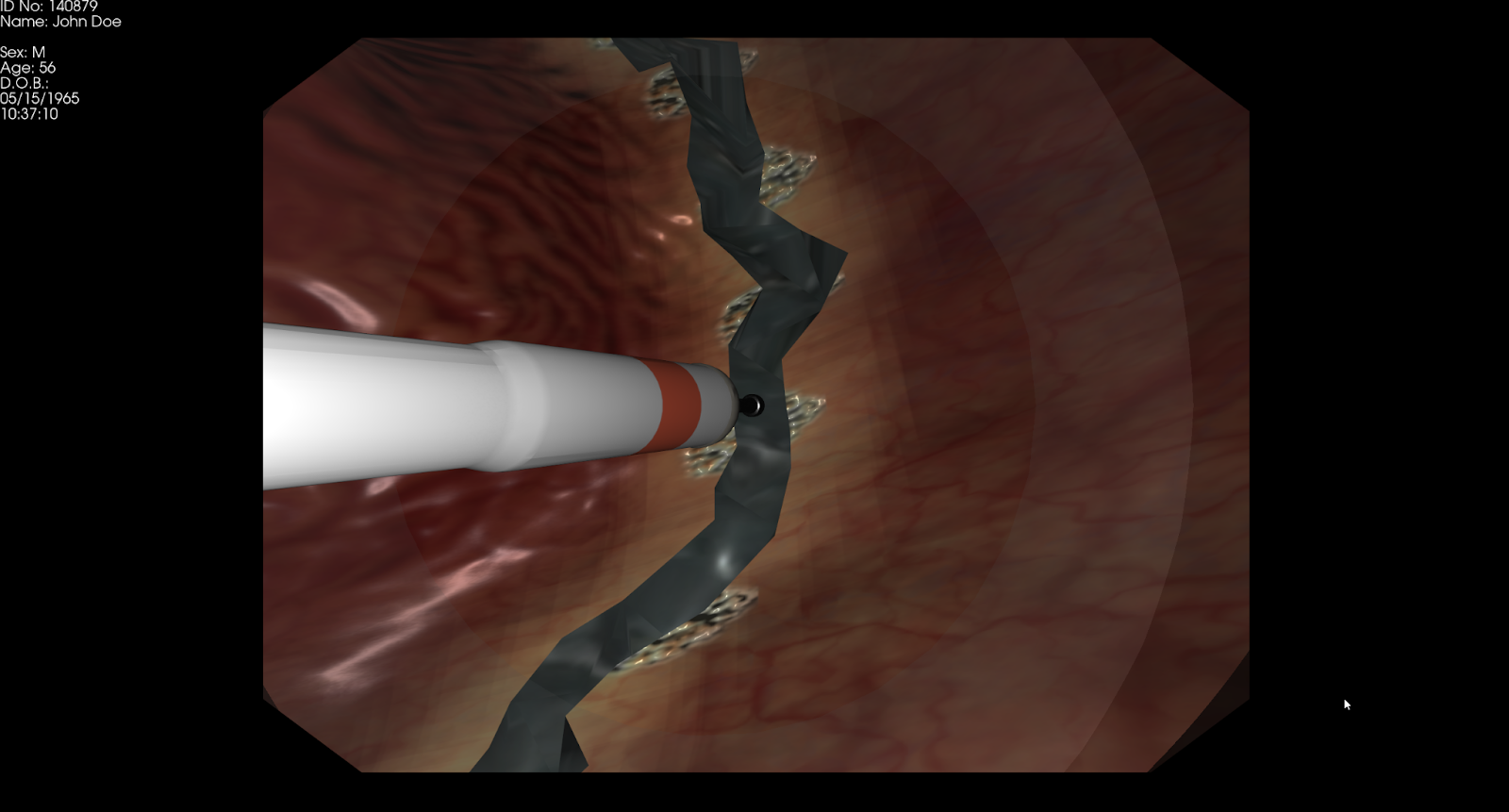
As part of the VESS, we modeled a patch of the colon tissue with which the tool may interact during the ESD procedure. Users can navigate to the site of the lesion and perform ESD following three main steps that were modeled in iMSTK:
- Marking: The marking stage involves using an electrosurgical instrument to mark the surface boundary of the lesion, which demarcates the area to be removed. In iMSTK, this was achieved by a simple alpha blend of a decal image onto the colon texture.
- Injection: Injection involves using a needle mounted on the endoscope to deliver blue fluid that inflates the submucosal layer beneath the lesion. This enlarges the inter-layer space, making it easier to remove and perform cutting. Additional injectant may be applied to maintain sufficient lift, as it spreads out during the procedure. Injection simulation was achieved by inflating the volume of the underlying tetrahedral elements proportional to the location in the Gaussian kernel around the tool tip.
- Dissection: After inflation, a mucosal circumferential incision is made using the electrosurgical knife following the boundary of the lesion. Then the submucosa below the tumor is dissected from the colon wall with the electrosurgical knife. During dissection the endoscopist cuts along the submucosa, being careful not to punch through the colon while removing the entirety of the tumor. Cutting in iMSTK was done via tetrahedral element removal. This method avoids buffer reallocation for fast cutting as it never adds/removes vertices in the mesh. The topology changes are locally tracked to avoid re-extracting the entire triangle surface mesh from the tetrahedral one for every update.
In addition to the above three surgical actions, VESS continuously detects any collision of the endoscope tube with the colon wall and simulates appropriate tissue response in real-time. Lastly, the software computes performance metrics that include the accuracy of dissection, total procedure time, and navigational skills as the user performs ESD.
The Future of VESS
VESS underwent several clinician feedback studies and is currently in the final phases of validation at Beth Israel Deaconess Medical Center in Boston. Once the validation studies are complete, CeMSIM, HMS, and Kitware will pursue extending the technology to other ESD procedures, such as peroral endoscopic myotomy, endomicroscopy for the diagnosis of functional and motility disorders, and peroral transgastric approaches to the peritoneum and mediastinum.
About Kitware’s Medical Computing Team
Kitware’s Medical Computing Team is composed of computer scientists, software engineers, and imaging experts who have been working with medical and biomedical customers for more than 20 years. We have domain expertise in surgical simulation and virtual surgery, image-guided intervention and surgical planning, and medical image analysis..We can provide support throughout your entire project, from determining feasibility to deploying solutions across a wide range of computing environments, to contributing to the regulatory submission. We operate as an extension of your team and truly get to know your specific challenges and needs. If you’re interested in learning more or would like to schedule a meeting with our Medical Computing Team, please email us at kitware@kitware.com.
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Number R01 CA197491. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.